
3.6: Amines as Neurotransmitters
- Page ID
- 227669
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Learning Objectives
- Describe how neurotransmitters work.
Amines have powerful biological functions. Many amines act as neurotransmitter and psychoactive drugs. These molecules generally produce their effects by affecting brain chemistry, which in turn may cause changes in a person’s mood, thinking, perception, and/or behavior. Each molecule tends to have a specific action on one or more neurotransmitters or neurotransmitter receptors in the brain. Generally, they act as either agonists or antagonists.
- Agonists are drugs that increase the activity of particular neurotransmitters. They might act by promoting the synthesis of the neurotransmitters, reducing their reuptake from synapses, or mimicking their action by binding to receptors for the neurotransmitters.
- Antagonists are drugs that decrease the activity of particular neurotransmitters. They might act by interfering with the synthesis of the neurotransmitters or by blocking their receptors so the neurotransmitters cannot bind to them.
Chemistry of the Nervous System
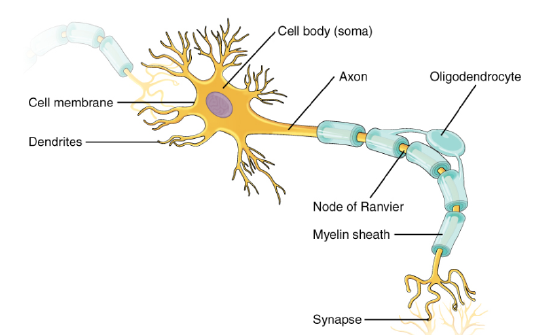 The brain and the rest of the nervous system are composed of many different types of cells, but the primary functional unit is a cell called the neuron (nerve cell) . All sensations, movements, thoughts, memories, and feelings are the result of signals that pass through neurons. Neurons consist of three parts (Figure \(\PageIndex{2}\)). The cell body contains the nucleus, where most of the molecules that the neuron needs to survive and function are manufactured. Dendrites extend out from the cell body like the branches of a tree and receive messages from other nerve cells. Signals then pass from the dendrites through the cell body and may travel away from the cell body down an axon to another neuron, a muscle cell, or cells in some other organ.
The brain and the rest of the nervous system are composed of many different types of cells, but the primary functional unit is a cell called the neuron (nerve cell) . All sensations, movements, thoughts, memories, and feelings are the result of signals that pass through neurons. Neurons consist of three parts (Figure \(\PageIndex{2}\)). The cell body contains the nucleus, where most of the molecules that the neuron needs to survive and function are manufactured. Dendrites extend out from the cell body like the branches of a tree and receive messages from other nerve cells. Signals then pass from the dendrites through the cell body and may travel away from the cell body down an axon to another neuron, a muscle cell, or cells in some other organ.
Scientists have learned a great deal about neurons by studying the synapse—the place where a signal passes from the neuron to another cell. When the signal reaches the end of 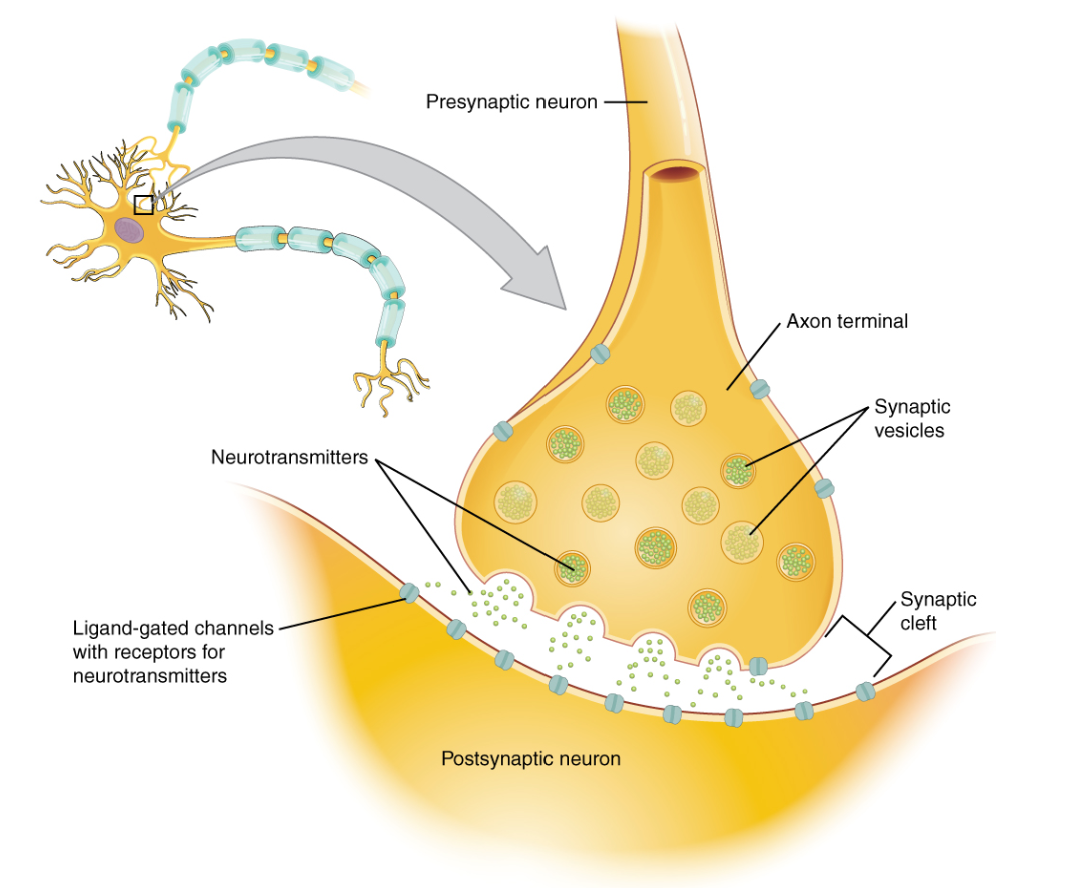 the axon it stimulates the release of tiny sacs. These sacs release chemicals called neurotransmitters into the synapse (Figure \(\PageIndex{3}\)) . The neurotransmitters cross the synapse and attach to receptors on the neighboring cell. These receptors can change the properties of the receiving cell. If the receiving cell is also a neuron, the signal can continue the transmission to the next cell.
the axon it stimulates the release of tiny sacs. These sacs release chemicals called neurotransmitters into the synapse (Figure \(\PageIndex{3}\)) . The neurotransmitters cross the synapse and attach to receptors on the neighboring cell. These receptors can change the properties of the receiving cell. If the receiving cell is also a neuron, the signal can continue the transmission to the next cell.
Neurotransmiters
Neurotransmitters are that enable . It is a type of chemical messenger which transmits signals across a , such as a , from one (nerve cell) to another "target" neuron.
Figure \(\PageIndex{3}\) The synapse. The synapse is a connection between a neuron and its target cell (which is not necessarily a neuron).
Biochemical Theories of Brain Diseases
The only direct action of a neurotransmitter is to activate a receptor. Therefore, the effects of a neurotransmitter system depend on the connections of the neurons that use the transmitter, and the chemical properties of the receptors that the transmitter binds to. An understanding of the functions of neurotransmitters (Table \(\PageIndex{1}\)) gives us a better idea of how an imbalance of these substances could contribute to certain brain disorders.
Strong imbalances or disruptions to neurotransmitter systems have been associated with many diseases and mental disorders. These include Parkinson's, depression, insomnia, Attention Deficit Hyperactivity Disorder (ADHD), anxiety, memory loss, dramatic changes in weight and addictions. Chronic physical or emotional stress can be a contributor to neurotransmitter system changes. Genetics also plays a role in neurotransmitter activities. Apart from recreational use, medications that directly and indirectly interact one or more transmitter or its receptor are commonly prescribed for psychiatric and psychological issues. Notably, drugs interacting with and are prescribed to patients with problems such as depression and anxiety—though the notion that there is much solid medical evidence to support such interventions has been widely criticized.
Monoamine Neurotransmitters: Serotonin, Dopamine, Epinephrine, and Norepinephrine
Monoamine neurotransmitters are and that contain one group connected to an ring by a two-carbon chain (such as -CH2-CH2-). Examples are , , norepinephrine and .
All monoamines are derived from aromatic like , , and by the action of . They are deactivated in the body by the enzymes known as which clip off the amine group.
 astrocytes, a chemical which maintains neuron integrity and provides neurons with trophic support.
astrocytes, a chemical which maintains neuron integrity and provides neurons with trophic support.

Figure \(\PageIndex{5}\) The biosynthesis of serotonin.
Barbiturates
Barbiturates are CNS depressants and are similar, in many ways, to the depressant effects of alcohol. To date, there are about 2,500 derivatives of barbituric acid of which only 15 are used medically. The first barbiturate was synthesized from barbituric acid in 1864.
The original use of barbiturates was to replace drugs such as opiates, bromides, and alcohol to induce sleep. Barbiturates are effective as , , and , but have physical and psychological potential as well as potential among other possible adverse effects. They have largely been replaced by (discussed below) and ("Z-drugs") in routine medical practice, particularly in the treatment of anxiety and insomnia, due to the significantly lower risk of addiction and and the lack of an for barbiturate overdose. Despite this, barbiturates are still in use for various purposes: in , , treatment of acute or , , , and .
![barbituates[1].gif](https://chem.libretexts.org/@api/deki/files/125061/barbituates%255B1%255D.gif?revision=1)
Some symptoms of an overdose typically include sluggishness, incoordination, difficulty in thinking, slowness of speech, faulty judgement, drowsiness, shallow breathing, staggering, and, in severe cases, coma or death. The lethal dosage of barbiturates varies greatly with tolerance and from one individual to another.
Barbiturates in overdose with other CNS (central nervous system) depressants (e.g. alcohol, opiates, benzodiazepines) are even more dangerous due to additive CNS and respiratory depressant effects. In the case of benzodiazepines, not only do they have additive effects, barbiturates also increase the binding affinity of the benzodiazepine binding site, leading to exaggerated benzodiazepine effects. (ex. If a benzodiazepine increases the frequency of channel opening by 300%, and a barbiturate increases the duration of their opening by 300%, then the combined effects of the drugs increase the channels overall function by 900%, not 600%).
Anti-anxiety Agents
Anti-anxiety medications help reduce the symptoms of anxiety, such as panic attacks, or extreme fear and worry.
The most common anti-anxiety medications are called benzodiazepines. Benzodiazepines can treat generalized anxiety disorder. In the case of panic disorder or social phobia (social anxiety disorder), benzodiazepines are usually second-line treatments, behind SSRIs or other antidepressants. Benzodiazepines used to treat anxiety disorders include, clonazepam (Klonopin), alprazolam (Niravam), and lorazepam (Altivam and Lorazepam Intensol).
Short half-life (or short-acting) benzodiazepines (such as Lorazepam) and beta-blockers are used to treat the short-term symptoms of anxiety. Beta-blockers help manage physical symptoms of anxiety, such as trembling, rapid heartbeat, and sweating that people with phobias (an overwhelming and unreasonable fear of an object or situation, such as public speaking) experience in difficult situations. Taking these medications for a short period of time can help the person keep physical symptoms under control and can be used “as needed” to reduce acute anxiety.
Antipsychotic medicines are primarily used to manage psychosis. The word “psychosis” is used to describe conditions that affect the mind, and in which there has been some loss of contact with reality, often including delusions (false, fixed beliefs) or hallucinations (hearing or seeing things that are not really there). It can be a symptom of a physical condition such as drug abuse or a mental disorder such as schizophrenia, bipolar disorder, or very severe depression (also known as “psychotic depression”).
Antipsychotic medications are often used in combination with other medications to treat delirium, dementia, and mental health conditions, including:
- Attention-Deficit Hyperactivity Disorder (ADHD)
- Severe Depression
- Eating Disorders
- Post-traumatic Stress Disorder (PTSD)
- Obsessive Compulsive Disorder (OCD)
- Generalized Anxiety Disorder
Antipsychotic medicines do not cure these conditions. They are used to help relieve symptoms and improve quality of life.
Older or first-generation antipsychotic medications are also called conventional "typical" antipsychotics or “neuroleptics”. Some of the common typical antipsychotics include, chlorpromazine (Promapar and Thorazine), haloperidol (Haldol), perphenazine (Trilafon), and fluphenazine (Permitil and Prolixin). Chlorpromazine was discovered in 1950 and was the first antipsychotic. It is on the , the most effective and safe medicines needed in a . Its introduction has been labeled as one of the great advances in the .
Chlorpromazine (CPZ), is marketed under the Thorazine and Largactil. It is primarily used to treat such as . Other uses include the treatment of , , and , anxiety before surgery, and that do not improve following other measures. It can be given by mouth, by , or . Common side effects include , , dry mouth, , and increased weight. Serious side effects may include the potentially permanent movement disorder , , and . In older people with psychosis as a result of it may increase the risk of death. It is unclear if it is safe for use in . Chlorpromazine is in the class. Its mechanism of action is not entirely clear but believed to be related to its ability as a .
Newer or second generation medications are called "atypical" antipsychotics. The atypical antipsychotics (AAP; also known as second generation antipsychotics (SGAs)) are a group of drugs (antipsychotic drugs in general are also known as major and neuroleptics, although the latter is usually reserved for the ) largely introduced after the 1970s and used to treat psychiatric conditions. Some atypical antipsychotics have received regulatory approval (e.g. by the of the , the of , the of the ) for , , , and as an in .Some of the common atypical antipsychotics include risperidone (Risperdal), olanzapine (Zyprexa), quetiapine (Seroquel), ziprasidone (Geodon), aripiprazole (Abilify), paliperidone (Invega), and lurasidone (Latuda). The atypical antipsychotics have found favor among clinicians and are now considered to be for schizophrenia and are gradually replacing the .
According to a 2013 research review by the Agency for Healthcare Research and Quality, typical and atypical antipsychotics both work to treat symptoms of schizophrenia and the manic phase of bipolar disorder. Several atypical antipsychotics have a “broader spectrum” of action than the older medications, and are used for treating bipolar depression or depression that has not responded to an antidepressant medication alone.
Older antidepressant medications include tricyclics, tetracyclics, and monoamine oxidase inhibitors (MAOIs). All tricyclic antidepressants in current use in the U.S. potentiate the actions of biogenic amines in the CNS by blocking its re-uptake at nerve terminals. However, the potency and selectivity for the inhibition of the uptake of norepinephrine, serotonin, and dopamine vary greatly among the agents. For some people, tricyclics, tetracyclics, or MAOIs may be the best medications.
The most popular types of antidepressants are called selective serotonin reuptake inhibitors (SSRIs) seeexamples on Figure \(\PageIndex{10}\) . Examples of SSRIs include fluoxetine (Prozac), citalopram (Celexa), sertraline (Zoloft), paroxetine (Brisdelle, Paxil, Pexeva), and escitalopram (Lexapro). Prozac is the most famous drug in this class. In 2016 it was the 29th most prescribed medication in the United States with more than 23 million prescriptions. Clomiprimine, fluoxetine (Prozac), sertraline and paroxetine selectively block the reuptake of serotonin, thereby increasing the levels of serotonin in the central nervous system. Some of the newer, SSRIs (e.g., clomipramine) have been useful in the treatment of obsessive-compulsive disorders.
![prozac[1].gif](https://chem.libretexts.org/@api/deki/files/125066/prozac%255B1%255D.gif?revision=1)
Other types of antidepressants are serotonin and norepinephrine reuptake inhibitors (SNRIs). SNRIs are similar to SSRIs and include venlafaxine (Effexor) and duloxetine (Cymbalta).
Another antidepressant that is commonly used is bupropion (Aplenzin, Wellbutrin, Wellbutrin SR, Wellbutrin XL) . Bupropion is a third type of antidepressant which works differently than either SSRIs or SNRIs. Bupropion is also used to treat seasonal affective disorder and to help people stop smoking.
SSRIs, SNRIs, and bupropion are popular because they do not cause as many side effects as older classes of antidepressants, and seem to help a broader group of depressive and anxiety disorders.
Cocaine, Caffeine, and Nicotine
Cocaine, also known as coke, is a strong most frequently used as a . It is commonly , inhaled as smoke, or dissolved and injected into a . Mental effects may include , an , or . Physical symptoms may include a , sweating, and .High doses can result in very or . Effects begin within seconds to minutes of use and last between five and ninety minutes. Cocaine has a small number of accepted medical uses such as and decreasing bleeding during nasal surgery.
Cocaine is due to its effect on the in the brain. After a short period of use, there is a high risk that will occur. Its use also increases the risk of , , lung problems in those who smoke it, , and . Cocaine sold on the street is commonly mixed with , cornstarch, , or sugar, which can result in additional toxicity. Following repeated doses a person may have and be very physically tired. Cocaine acts by
Caffeine is a (CNS) of the . Caffeine is a stimulant compound belonging to the class of chemicals naturally found in , , and (to a lesser degree) or . It is included in many , as well as a larger amount in . Caffeine is the world's most widely used psychoactive drug and by far the most common stimulant. In North America, 90% of adults consume caffeine daily. A few jurisdictions restrict its sale and use. Caffeine is also included in some medications, usually for the purpose of enhancing the effect of the primary ingredient, or reducing one of its side-effects (especially drowsiness). Tablets containing standardized doses of caffeine are also widely available.
Caffeine's mechanism of action differs from many stimulants, as it produces stimulant effects by inhibiting adenosine receptors. Adenosine receptors are thought to be a large driver of drowsiness and sleep, and their action increases with extended wakefulness. Caffeine (in coffee), theophylline (in tea) and theobromine (in choccolate) share in common several pharmacological actions of therapeutic interest. They stimulate the central nervous system, act on the kidney to produce diuresis, stimulate cardiac muscle, and relax smooth muscle, notably bronchial muscle. From the figure below, we can see that the methylxanthines have a structure which is very similar to adenine (the amino group in adenosine).
![cafeine[1].gif](https://chem.libretexts.org/@api/deki/files/125067/cafeine%255B1%255D.gif?revision=1)
is the active chemical constituent in , which is available in many forms, including , , , and aids such as , , and . Nicotine is used widely throughout the world for its stimulating and relaxing effects. Nicotine exerts its effects through the agonism of , resulting in multiple downstream effects such as increase in activity of dopaminergic neurons in the midbrain , as well as the decreased expression of in the brain. Nicotine is addictive and dependence forming.
Hallucinogens and Dissociative Drugs
 feeling sensations that seem real but are not. While the exact mechanisms by which hallucinogens and dissociative drugs cause their effects are not yet clearly understood, research suggests that they work at least partially by temporarily disrupting communication between neurotransmitter systems throughout the brain and spinal cord that regulate mood, sensory perception, sleep, hunger, body temperature, sexual behavior, and muscle control.
feeling sensations that seem real but are not. While the exact mechanisms by which hallucinogens and dissociative drugs cause their effects are not yet clearly understood, research suggests that they work at least partially by temporarily disrupting communication between neurotransmitter systems throughout the brain and spinal cord that regulate mood, sensory perception, sleep, hunger, body temperature, sexual behavior, and muscle control.
are commonly used hallucinogenic and dissociative compounds.
Classic Hallucinogens
LSD (d-lysergic acid diethylamide)—also known as acid, blotter, doses, hits, microdots, sugar cubes, trips, tabs, or window panes—is one of the most potent moodand perception-altering hallucinogenic drugs. It is a clear or white, odorless, water-soluble material synthesized from lysergic acid, a compound derived from a rye fungus. LSD is initially produced in crystalline form, which can then be used to produce tablets known as “microdots” or thin squares of gelatin called “window panes.” It can also be diluted with water or alcohol and sold in liquid form. The most common form, however, is LSD-soaked paper punched into small individual squares, known as “blotters.”
Psilocybin (4-phosphoryloxyN, N-dimethyltryptamine)—also known as magic mushrooms, shrooms, boomers, or little smoke—is extracted from certain types of mushrooms found in tropical and subtropical regions of South America, Mexico, and the United States. In the past, psilocybin was ingested during religious ceremonies by indigenous cultures from Mexico and Central America. Psilocybin can either be dried or fresh and eaten raw, mixed with food, or brewed into a tea, and produces similar effects to LSD.
Peyote (Mescaline)— also known as buttons, cactus, and mesc— is a small, spineless cactus with mescaline as its main ingredient. It has been used by natives in northern Mexico and the southwestern United States as a part of religious ceremonies. The top, or “crown,” of the peyote cactus has disc-shaped buttons that are cut out, dried, and usually chewed or soaked in water to produce an intoxicating liquid. Because the extract is so bitter, some users prepare a tea by boiling the plant for several hours. Mescaline can also be produced through chemical synthesis.
DMT (Dimethyltryptamine)—also known as Dimitri—is a powerful hallucinogenic chemical found naturally occurring in some Amazonian plant species (see “Ayahuasca”) and also synthesized in the laboratory. Synthetic DMT usually takes the form of a white crystalline powder and is typically vaporized or smoked in a pipe. Ayahuasca—also known as hoasca, aya, and yagé—is a hallucinogenic brew made from one of several Amazonian plants containing DMT (the primary psychoactive ingredient) along with a vine containing a natural alkaloid that prevents the normal breakdown of DMT in the digestive tract. Ayahuasca tea has traditionally been used for healing and religious purposes in indigenous South American cultures, mainly in the Amazon region.
Dissociative Drugs
PCP (Phencyclidine)—also known as ozone, rocket fuel, love boat, hog, embalming fluid, or superweed—was originally developed in the 1950s as a general anesthetic for surgery. While it can be found in a variety of forms, including tablets or capsules, it is usually sold as a liquid or powder. PCP can be snorted, smoked, injected, or swallowed. It is sometimes smoked after being sprinkled on marijuana, tobacco, or parsley.
Ketamine—also known as K, Special K, or cat Valium—is a dissociative currently used as an anesthetic for humans as well as animals. Much of the ketamine sold on the street has been diverted from veterinary offices. Although it is manufactured as an injectable liquid, ketamine is generally evaporated to form a powder that is snorted or compressed into pills for illicit use. Because ketamine is odorless and tasteless and has amnesia-inducing properties, it is sometimes added to drinks to facilitate sexual assault. 2 NIDA Research Report Series Common Hallucinogens and Dissociative Drugs *In this report, the term “hallucinogen” will refer to the classic hallucinogenic drugs LSD and Psilocybin.
DXM (Dextromethorphan)— also known as robo—is a cough suppressant and expectorant ingredient in some over-the-counter (OTC) cold and cough medications that are often abused by adolescents and young adults. The most common sources of abused DXM are “extra-strength” cough syrup, which typically contains around 15 milligrams of DXM per teaspoon, and pills and gel capsules, which typically contain 15 milligrams of DXM per pill. OTC medications that contain DXM often also contain antihistamines and decongestants.
Salvia divinorum—also known as diviner’s sage, Maria Pastora, Sally-D, or magic mint—is a psychoactive plant common to southern Mexico and Central and South America. Salvia is typically ingested by chewing fresh leaves or by drinking their extracted juices. The dried leaves of salvia can also be smoked or vaporized and inhaled.
Short-Term General Effects of Hallucinogens Sensory Effects
• Hallucinations, including seeing, hearing, touching, or smelling things in a distorted way or perceiving things that do not exist
• Intensified feelings and sensory experiences (brighter colors, sharper sounds)
• Mixed senses (“seeing” sounds or “hearing” colors)
• Changes in sense or perception of time (time goes by slowly) Physical Effects
• Increased energy and heart rate
• Nausea
Summary
- Neurotransmitters are that enable . It is a type of chemical messenger which transmits signals across a , such as a , from one (nerve cell) to another "target" neuron, , or .
- Strong imbalances or disruptions to neurotransmitter systems have been associated with many diseases and mental disorders.
- Psychoactive drugs are substances that change the function of the brain and result in alterations of mood, thinking, perception, and/or behavior. They include prescription medications such as opioid painkillers, legal substances such as nicotine and alcohol, and illegal drugs such as LSD and heroin.
- Psychoactive drugs are divided into different classes according to their pharmacological effects. They include stimulants, depressants, anxiolytics, euphoriants, hallucinogens, and empathogens. Many psychoactive drugs have multiple effects so they may be placed in more than one class.
- Psychoactive drugs generally produce their effects by affecting brain chemistry. Generally, they act either as agonists, which enhance the activity of particular neurotransmitters; or as antagonists, which decrease the activity of particular neurotransmitters.
- Psychoactive drugs are used for various purposes, including medical, ritual, and recreational purposes.
- Misuse of psychoactive drugs may lead to addiction, which is compulsive use of a drug despite negative consequences such use may entail. Sustained use of an addictive drug may produce physical or psychological dependence on the drug. Rehabilitation typically involves psychotherapy and sometimes the temporary use of other psychoactive drugs.
Sources
NIH National Institute of Neurological Disorder and Stroke (NIDS)
NIH National Institute of Mental Health
NIH National Institute on Drug Abuse
Wikipedia
Contributors and Attributions
- Libretext: Human Biology (Wakim and Grewal)
- Charles Ophardt, Professor Emeritus, Elmhurst College; Virtual Chembook
- Psychology OPENSTAX
- Drugs and the Mind. (2020, August 13). Retrieved May 23, 2021, from https://chem.libretexts.org/@go/page/153917