
4.27: Creatine Kinase (CK) Isoenzymes
- Page ID
- 122419

A series of three samples is sent to the Chemistry Laboratory with a request for a “cardiac profile”. All three samples are analyzed for total CK and have results >8000 U/L. It is noted that the samples are colored orange-green. The laboratory routinely analyzes all samples with elevated CK values for CK-MB, but the technologist is not quite sure if the immunoinhibition assay technique in use will work on samples with such elevated levels of CK or on ones which are so highly colored. The patient is a 44-year-old Caucasian female who was transferred to the hospital two days before from a community hospital. The patient was placed in the Medical Intensive Care Unit (MICU). After the technologist discusses the problem with the laboratory’s clinical chemist, the decision is made to perform CK isoenzyme analysis by electrophoresis rather than by the immunoinhibition assay. The results are described schematically below:
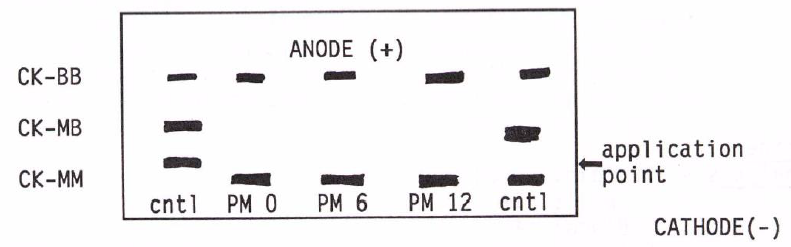
Where PM 0, 6, and 12 are the samples drawn at 0, 6, and 12 hours after admission. The technologist, concerned that this unusual pattern might be the result of technical or specimen collection errors, reviews the data with the laboratory’s clinical chemist.
QUESTION
What clinical problems could cause this CK isoenzyme profile?
In order to determine the nature of the patient’s disease, the clinical chemist and the technologist review other laboratory data on the patient.
Some other laboratory values obtained that day on that patient included:
| Na | 134 mmol/L |
| K | 7.0 mmol/L |
| BUN | 570 mg/L |
| Creatinine | 24 mg/L |
| Glucose | 1260 mg/L |
| Anion gap | 24 mmol/L |
| Lactic acid | 25.2 mmol/L |
| Calcium | 91 mg/L |
| Inorganic phosphorous | 101 mg/L |
| Total bilirubin | 229 mg/L |
| Direct bilirubin | 110 mg/L |
| ALT (SGPT) | 2270 U/L |
| AST (SGOT) | 9710 U/L |
| Alk phosphatase (AP) | 3950 U/L |
| 5' nucleotidase | 130 U/L |
| Protein | 3000 mg/L |
| Bili | 4+ |
| Blood | 4+ |
| Nitrite | pos |
| WBC/RBC | TNTC |
| Bacteria | 3+ |
(Reference intervals for many of these analyses are found inside the front and back covers of the 4th Edition and in the CD-ROM.)
In addition, the patient had a raised WBC and a markedly low RBC; Hb = 104 g/L. Platelet count was abnormally low; PT/PTT were 23 and 55 seconds, both markedly elevated; with FDP (fibrin degradation products) almost 20-fold elevated (256 mg/L). Serology for hepatitis were all negative; the patient had never been infected with hepatitis virus.
QUESTION
Which disease would be most likely to cause these laboratory results and the CK isoenzyme pattern?
Questions to Consider
- What organs are major sources of CK-MM? CK-MB? CK-BB?
- Are there any other electrophoretic variant forms of CK? If so, what are they?
- Are there any common laboratory or sample collection errors that could cause such a CK pattern?
- Which of the laboratory results are most unusual? What type of diseases is suggested by these results?
- What are some causes of an increased serum lactic acid?
- Why was the sample so unusually colored?
- The original request was for a 'cardiac profile'; what other tests can be ordered to determine if this patient had cardiac damage?
- Answer
-
- Heart has the highest percentage and levels of CK-MB, although certain types of muscle fiber can also have high levels of CK-MB. The brain and colon have the highest levels of CK-BB activity, although lung tissue can often be a source of serum CK-BB.
- The troponin I assay was run on all the samples and was not detected in all cases.
The most likely explanation for the atypical CK electrophoretogram is some cancer, either lung or colon, which has metastasized to the liver. Since certain types of very aggressive lung tumors (oat cell carcinomas) often produce large amounts of CK-BB, lung cancer is most likely. Extensive metastasizing of the primary tumor to the liver would destroy the liver and would explain the large increases in AP, LD, 5’-nucleotidase, bilirubin, and bile acids (Chapter 27). The severe lactic acidemia is most likely caused by the rapid metabolism of the anoxic tumor, made worse by the diminished capacity of the liver to remove lactic acid from the blood.
It should be noted that the most likely explanation for a severely atypical CK electrophoretogram is cancer.
Note
This patient died within 72 hours of hospitalization of severe liver metastasis from a primary oat cell carcinoma of the lung.)
Answers to Questions to Consider
- Skeletal muscle is the major source of CK-MM in terms of percentage of total CK and absolute units of activity per gram of tissue (Table 55-1, p 1067).
- There are two types of rarely seen isoenzyme forms of CK. They are the mitochondrial CK (mCK) and macro-CK forms. The latter may be complexes between CK and antibodies to CK (see Methods on CD-ROM CK isoenzymes ). While the mCK activity is found at a slightly cathodic position on agarose electrophoresis, the macro-CK activities can be found in unusual positions anywhere in the electrophoretogram.
SEE Web sites: www.labcorp.com/datasets/labc...o/sc005800.htm
puma.protein.bio.msu.su/biokh...f/bcm_1098.pdf
www.gpnotebook.co.uk/cache/1322254395.htm
www.ncbi.nlm.nih.gov/htbin-po...=r&uid=8013099 - There are no known sample collection problems or technical errors that would result in such a pattern. Large amounts of total CK, with increased amounts of CK-BB and the presence of an atypical anodic band of mCK activity might be associated with disease of some organ containing large amounts of CK-BB, that is severe disease of the brain, colon, lung, or in men, prostate. In addition, one would have to consider the presence of some cancer since large amounts of CK-BB may be produced by some cancers (Chapter 55).
Large amounts of CK-BB might prompt an acute immunological response by the patient with the resulting formation of Ig-CK-BB complexes that might migrate cathodically. The alternate explanation for the atypical cathodic band is mCK, which is often found in very acute terminal illnesses. - Certainly the most striking of these results are the extraordinarily large increases of LD, CK, and AST. The elevated levels of creatinine and BUN and the results of the urine analysis certainly demonstrate the presence of a protein-losing nephropathy (Tables 26-2 and 26-3 of the 4th Edition,). Elevated levels of the transaminases, bilirubin, and alkaline phosphatase are indications of a fairly severe liver disease.
- Lactic acid is produced in large amounts by anoxic tissues, that is, tissues with very low oxygen levels (p. 471). This can be the result of general circulatory collapse with diminished oxygen delivery, or the result of increased oxygen consumption by tissues (fever, prolonged exercise, or rapidly metabolizing tumors). Further increases in serum lactic acid can be caused by a diseased liver which can no longer clear lactic acid from the blood.
- The highly colored serum is most likely caused by large amounts of bile acids; probably the result of the severe liver dysfunction (p 497).
- The best test to rule out cardiac damage would be a troponin (I or T) assay (see p. 576-577). These assays are now routinely available in most hospitals.